Fusions
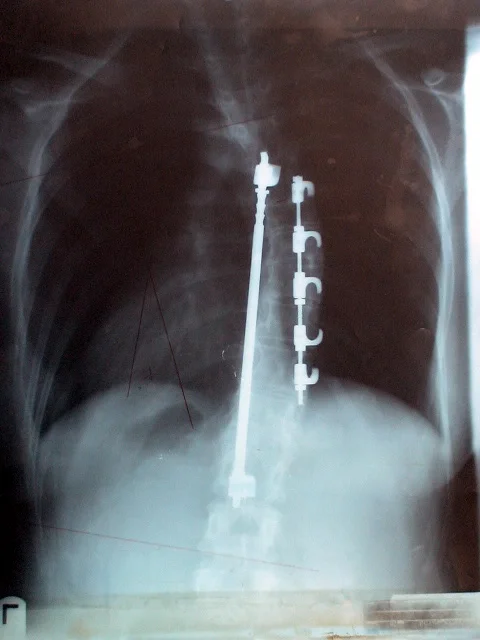
Surgical techniques used to correct scoliotic spines are changing and evolving all the time. We’ve included a very brief overview of the most common approaches, with some descriptions and pictures to help illustrate some of the different techniques.
It is important to note that this is not a complete list and that each method has its own variations.
It is also important to remember that different techniques are used / recommended for particular reasons - whether it’s the type of curve, the speed of the progression, the age and health of the patient, or the specific specialties of the surgeon. It is highly recommended that anyone considering surgery get at least two medical opinions in order to have enough information to consider all of the possible options before deciding which approach might be most suitable for them.
I want to thank the many internet sources that assisted me in my journey of researching and compiling this list over time. I would also like to thank the many friends and colleagues who helped me with additional information and images, including several Scoliosis warriors from Facebook who offered up their x-rays, as well as Nancy DL Heraty, Yoga teacher, Scoliosis specialist, and co-author with Elise Browning Miller of the wonderful book, Yoga for Scoliosis: A Path for Students and Teachers.